

Talking — Here’s How to Know
Most stomach aches are nothing. But appendicitis is the one you really don’t want to miss.
Here’s how to recognise it, what doctors look for, and why acting fast matters.
Your Appendix: Small Organ, Big Problem
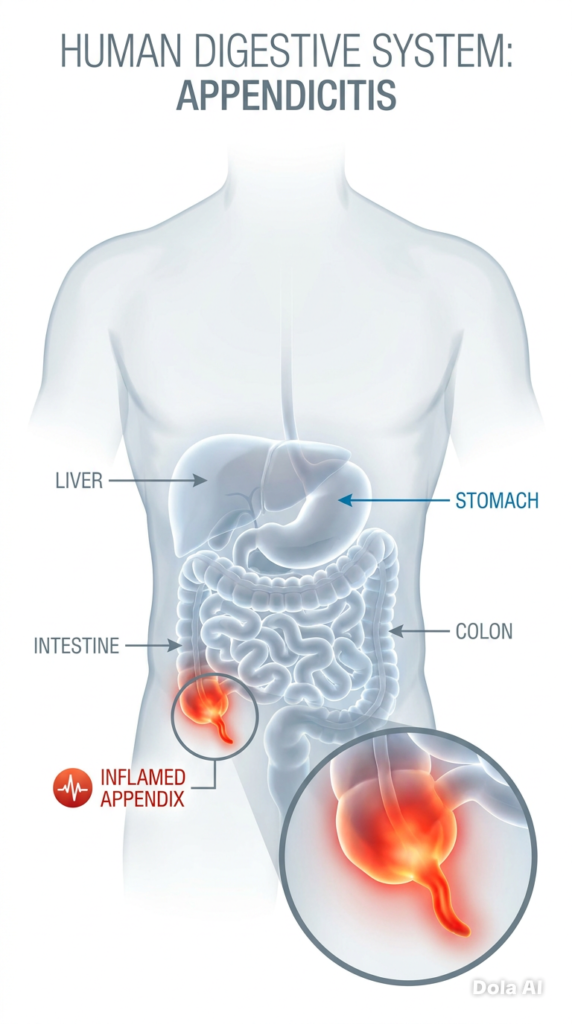
Tucked away in the lower right corner of your abdomen sits a small, worm-shaped structure
called the appendix. For most of your life, it does absolutely nothing of note. But when it
becomes blocked — whether by hardened stool, mucus, or infection — it rapidly becomes
the most inconvenient organ in your body.
The blockage triggers inflammation. The inflamed appendix swells. If nobody intervenes, it
can burst — spilling bacteria into the abdominal cavity and turning a manageable situation
into a life-threatening one.
Appendicitis strikes roughly 1 in every 13 people during their lifetime, making it one of the
most common reasons people end up in emergency surgery. It has a particular fondness for
teenagers and young adults, though it will happily affect anyone from toddlers to
pensioners.
The reassuring part: caught before it ruptures, appendicitis is one of the most
straightforward surgical emergencies to treat. The tricky part: its symptoms can be
deceptively ordinary at first.
The Way Appendicitis Pain Behaves Is Unlike Most Stomach
Aches
Here is the thing about appendicitis — it rarely announces itself with drama right from the
start. It tends to creep up on you.
It Starts Somewhere Unexpected
Before the pain settles in the lower right abdomen (where your appendix actually lives), it
typically begins around your belly button. This catches many people off guard. They assume
it is a stomach bug, trapped wind, or something they ate. The ache is dull and hard to pin
down — almost like a general sense of abdominal unease rather than a sharp, obvious pain.
Then It Moves — and Stays
Over the following hours, something distinctive happens. The pain travels. It shifts from
around the navel and settles firmly in the lower right side of the abdomen, in an area doctors
call the right iliac fossa. Once it arrives there, it tends to stay put and intensify rather than
come and go in waves the way period cramps or food poisoning might.
Pressing on that area hurts. So does sneezing, coughing, going over a speed bump, or even
walking. Many people find themselves instinctively hunching to one side or shuffling rather
than striding — unconsciously guarding that tender spot.
Food Becomes the Last Thing on Your Mind
Long before the pain becomes severe, the appetite quietly disappears. This is one of the
earliest and most consistent features of appendicitis — an almost total disinterest in eating,
even foods you would usually enjoy. It is not just feeling too sore to eat; it is a genuine loss
of desire.
Nausea follows, and sometimes vomiting. One detail worth knowing: with appendicitis, the
stomach upset tends to come after the pain begins — not before. If you were sick first and
the pain came later, something else may be going on.
A Fever That Builds
A mild temperature — typically between 37.5°C and 38.5°C — develops as the body
responds to the inflammation. It is easy to dismiss this as the beginning of a cold or flu,
especially alongside the nausea. But paired with the lower right abdominal pain, it becomes
a much more meaningful clue.
A temperature above 39°C is a warning sign that the situation may be escalating.
Bowel Changes You Might Not Expect
Appendicitis can disrupt normal bowel habits in either direction. Constipation is more
common — some people find they simply cannot go. Others, particularly when the appendix
sits in a position close to the bowel or pelvis, experience loose stools or an urgent need to
go. Neither is definitive on its own, but both are worth noting alongside other symptoms.
Why Appendicitis Does Not Always Feel the Same for Everyone
This is where appendicitis earns its reputation as a “great imitator.” The textbook description
above applies to many people — but not all.
Women face a particular diagnostic challenge. The lower right abdomen is shared territory:
the appendix lives alongside the ovary and fallopian tube on that side. Appendicitis can look
remarkably similar to ovarian cysts, a twisted ovary, pelvic inflammatory disease, or — most
urgently — an ectopic pregnancy. Doctors will always consider these possibilities, and
additional tests are almost always performed in women.
Children often cannot articulate where exactly they hurt. They may simply seem irritable,
refuse meals, clutch their tummy, or be reluctant to walk or jump. Parents sometimes bring
children in for what looks like a stomach bug, only for appendicitis to be discovered. Trust
your instincts if your child seems more unwell than a typical tummy ache warrants.
Older adults can experience a muted version of the classic symptoms — less dramatic pain,
a lower fever, fewer obvious warning signs. This makes appendicitis easier to miss and often
means a more advanced stage by the time it is diagnosed.
During pregnancy, the growing uterus physically pushes the appendix upward and to the
right. Pain may be felt higher in the abdomen than expected, around the mid-right side
rather than the lower right. This displacement is one reason appendicitis during pregnancy
can be particularly challenging to diagnose.
When You Must Act Immediately — Call 999 or Go Straight to
A&E
Some symptoms mean there is no time to wait for a GP appointment or to see if things
improve overnight.
Seek emergency help without delay if:
The abdominal pain suddenly becomes severe and spreads across the entire abdomen
— this can signal the appendix has burst
The abdomen feels rigid or board-like to the touch — a sign of widespread inflammation
called peritonitis
You develop a very high fever (above 39°C) alongside abdominal pain
You feel faint, dizzy, or your heart is racing — signs the body is under serious stress
Vomiting is persistent and nothing stays down
A ruptured appendix is a genuine emergency. The mortality risk rises sharply once rupture
occurs — but with prompt treatment, outcomes remain good. Do not wait to see how things
develop.
What Happens at the Hospital: The Tests Doctors Use
If you arrive at hospital with suspected appendicitis, you will not simply be wheeled into
surgery based on your symptoms alone. Diagnosis involves a structured sequence of
examination and investigation — because several other conditions can produce nearly
identical symptoms and ruling them out matters enormously.
The Hands-On Examination
Before any blood is drawn or scans requested, a doctor will examine your abdomen. This is
not a formality — skilled examination can tell an experienced clinician a great deal. They are
looking for:
McBurney’s point tenderness. There is a specific anatomical landmark — roughly one-
third of the way along a line drawn from your right hip bone to your navel. Pinpoint
tenderness here is a classic indicator.
Rebound tenderness. The doctor presses firmly and then releases suddenly. If the release
hurts more than the pressing, the peritoneum (the lining of the abdominal cavity) is irritated
— a significant finding.
Rovsing’s sign. Here is the counterintuitive one: pressing on the left side of the abdomen
provokes pain on the right. This occurs because pressure shifts the contents of the bowel
and irritates the inflamed appendix from a distance.
Guarding. When the abdomen is touched, the muscles beneath automatically tense and
resist — the body’s involuntary attempt to protect the inflamed area. Voluntary guarding
(tensing on purpose because it hurts) is different from involuntary guarding (the muscles
contract before the patient can stop them).
Psoas and obturator signs. Specific movements of the hip can provoke or worsen the pain
depending on exactly where the appendix sits. These signs help surgeons understand the
appendix’s position before imaging confirms it.
Blood Tests: The Body’s Internal Report Card
Bloods are drawn early and tell the team a great deal about what is happening internally.
A full blood count (FBC) checks the white cell count. An elevated count — particularly a
surge in neutrophils, the white cells that fight bacterial infection — strongly suggests
something inflammatory is occurring. It does not confirm appendicitis on its own, but it
raises the index of suspicion considerably.
C-reactive protein (CRP) is a protein the liver releases in response to inflammation
anywhere in the body. A raised CRP adds weight to the clinical picture. Very high levels can
suggest the inflammation is advanced or that rupture may have already occurred.
Urea, electrolytes, and kidney function are checked to ensure hydration is adequate and
the kidneys are coping — important before surgery and when IV fluids may be needed.
Liver function tests and amylase or lipase help exclude other abdominal culprits —
gallbladder disease, bile duct problems, and pancreatitis can all produce right-sided or
central abdominal pain that superficially resembles appendicitis.
Urine Test: Ruling Out the Mimics
A urine dipstick is among the first tests performed. Urinary tract infections are extremely
common and can cause lower abdominal pain and general unwellness that overlap with
appendicitis. Kidney stones cause severe abdominal and flank pain that can occasionally
confuse the picture. Both are quickly identifiable on urine testing and easily distinguished
from appendicitis once the result is in.
Pregnancy Test: Always Done in Women of Childbearing Age
An ectopic pregnancy — where a fertilised egg implants in the fallopian tube rather than the
uterus — is a medical emergency that can mimic appendicitis almost perfectly, including the
location of the pain. It can rupture and cause life-threatening internal bleeding. A simple
urine or blood β-hCG test identifies pregnancy within minutes and is done routinely
regardless of whether the patient believes they could be pregnant.
Imaging: Seeing Inside to Be Sure
When examination and blood tests leave any uncertainty — which is surprisingly often, given
how closely appendicitis can resemble other conditions — imaging provides a clearer
picture.
Ultrasound is the starting point, particularly for children and pregnant women. It involves no
radiation, is widely available, and can often identify an inflamed appendix along with other
nearby structures. Its limitation is that it depends on the skill of the operator and the
patient’s body habitus — bowel gas and a larger frame can make the appendix difficult to
see clearly.
CT scanning of the abdomen and pelvis is the most accurate single investigation
available, with sensitivity approaching 95%. It can visualise the appendix directly, confirm
inflammation, detect perforation, and simultaneously identify alternative diagnoses if
appendicitis turns out not to be the cause. It involves a small dose of ionising radiation,
which is why it tends to be reserved for adults where ultrasound is inconclusive or the
clinical picture is complex.
MRI steps in where CT would be inappropriate — most often in pregnant women where
avoiding radiation is a priority. It is slower, less immediately available, and more expensive,
but produces excellent soft tissue detail without any radiation exposure.
Plain abdominal X-ray has a very limited role. Appendicitis itself is essentially invisible on a
standard X-ray. Occasionally a hardened deposit called a faecolith — essentially a calcified
lump that may have triggered the blockage — shows up, but this is the exception. X-rays are
more useful for ruling out bowel obstruction or perforation.
Scoring Systems: Turning Symptoms Into Numbers
Clinicians do not rely solely on instinct. Several validated scoring tools have been developed
to combine symptoms, examination findings, and blood test results into a numerical score
that helps guide the next step.
The Alvarado score is the most widely used. It awards points for key features — the typical
pain migration, nausea, fever, tenderness at McBurney’s point, rebound tenderness, a raised
white cell count, and a shift toward neutrophils. Scores of 1–4 suggest low risk. Scores of 5–
6 sit in an intermediate zone where further imaging is usually warranted. A score of 7 or
above indicates a high likelihood of appendicitis and typically prompts urgent surgical
review.
The MANTA score is a newer tool adopted in some UK centres specifically to guide the
decision of whether imaging is necessary before referring to a surgeon.
Treatment: What Comes After Diagnosis
Once appendicitis is confirmed, the appendix comes out. The procedure — an
appendicectomy — is one of the most commonly performed emergency operations in the
country. The vast majority are done laparoscopically (keyhole surgery), using small incisions
and a camera, under general anaesthetic. Most people are home within 24 to 48 hours.
Open surgery is occasionally necessary, particularly if the appendix has already ruptured
and the surgeon needs better access to clean the abdominal cavity.
There is growing evidence that in carefully selected cases of uncomplicated appendicitis —
where the appendix has not burst and there are no complicating features — a course of
intravenous antibiotics can treat the condition without surgery. This approach is increasingly
offered as an option and discussed with patients. However, there is a meaningful chance of
the appendicitis recurring, and surgery remains the only definitive cure.
Recovery from keyhole surgery is typically straightforward: most people are back to desk
work within one to two weeks and fully active within four to six weeks.
The Bottom Line on When to Get Help
Appendicitis is not the kind of thing to “wait and see” with. The window between early
inflammation and rupture is typically 24 to 72 hours — and that window is not predictable.
Some appendices perforate faster.
Contact your GP or call NHS 111 if:
You have had persistent right-sided abdominal pain for more than a few hours
The pain is accompanied by nausea, fever, or a complete loss of appetite
Something feels wrong and you cannot shake the feeling
Go directly to A&E or call 999 if:
The pain has become severe, is spreading, or is no longer localised
Your abdomen feels hard or rigid
You have a high fever, are vomiting repeatedly, or feel faint
No doctor will ever think less of you for coming in with abdominal pain that turns out to be
nothing serious. But arriving early with appendicitis rather than late makes every part of
what follows simpler, safer, and faster.
Quick Reference: Key Points to Remember
Appendicitis pain classically begins near the belly button before travelling to the lower
right abdomen — and it gets worse, not better, over time
Loss of appetite and nausea come early; the nausea follows the pain rather than
preceding it
Fever, tenderness on the right side, and an elevated white cell count together are
powerful indicators
Diagnosis combines physical examination, blood tests, urine tests, and often ultrasound
or CT scanning
Treatment is almost always surgical; most people recover fully within weeks
The earlier it is caught, the simpler and safer the treatment is.
This article is intended for general health information only and is not a substitute for
professional medical advice, diagnosis, or treatment. If you have concerns about your
symptoms, please contact your GP, call NHS 111, or attend your nearest A&E department.


